When Silence Should Be Screaming, but Perhaps It Was Masked Too — Alarming Google Trends Data and the Cornerstone of Deception: the Mask
HUNGARIAN: Amikor a csend üvöltene, de lehet, arra is maszkot húztak – A Google Trends riasztó adatai és a hazugságok alapköve: a maszk
MAGYAR VERZIÓ IDE KATTINTVA OLVASHATÓ.
Over the past weeks, the silence on my page has not been accidental. Many of us — myself included — have recently felt that while answers and explanations are steadily coming to light, things on the surface still continue along the same course, as if nothing had happened.
The “noise” of this cognitive dissonance became so deafening for me that
I needed to take a short break.
Day after day, the “explanations” of the mainstream media are poured over us. You surely see the headlines as well, in which “experts” explain why it is supposedly natural that healthy people collapse on sports fields, or why more and more young people are suffering heart attacks. The list of culprits grows longer by the day: climate change, cold weather, hot weather, too much gardening, suddenly getting out of bed, or even overly intense emotions. Everything is declared dangerous, an explanation is found for everything — except for one thing. The elephant in the room, which is not only forbidden to talk about, but even to ask about, or so much as allude to.
And while official communication insists that “everything is fine”, and “sudden death” becomes the new normal, reality forces its way to the surface beneath it all. Not in the news broadcasts, but in the one place where people do not lie: the Google search engine…
Take a look at what is happening to the Google Trends data.
For those who may not be familiar with it: Google Trends is the world’s largest search data repository, which shows in black and white what people are actually searching for on their private devices. This statistic does not lie and does not beautify reality; it reveals the unfiltered, collective symptoms of society — what millions are worried about behind closed doors, regardless of what the news broadcasts say.
An important technical detail: the 0–100 scale shown on the graphs does not represent absolute numbers. A value of 100 marks the historical peak of interest, while 0 means that activity during that period was negligible compared to the peak. The curves therefore do not represent “100 people,” but rather a relative, explosive increase in interest in the issue.
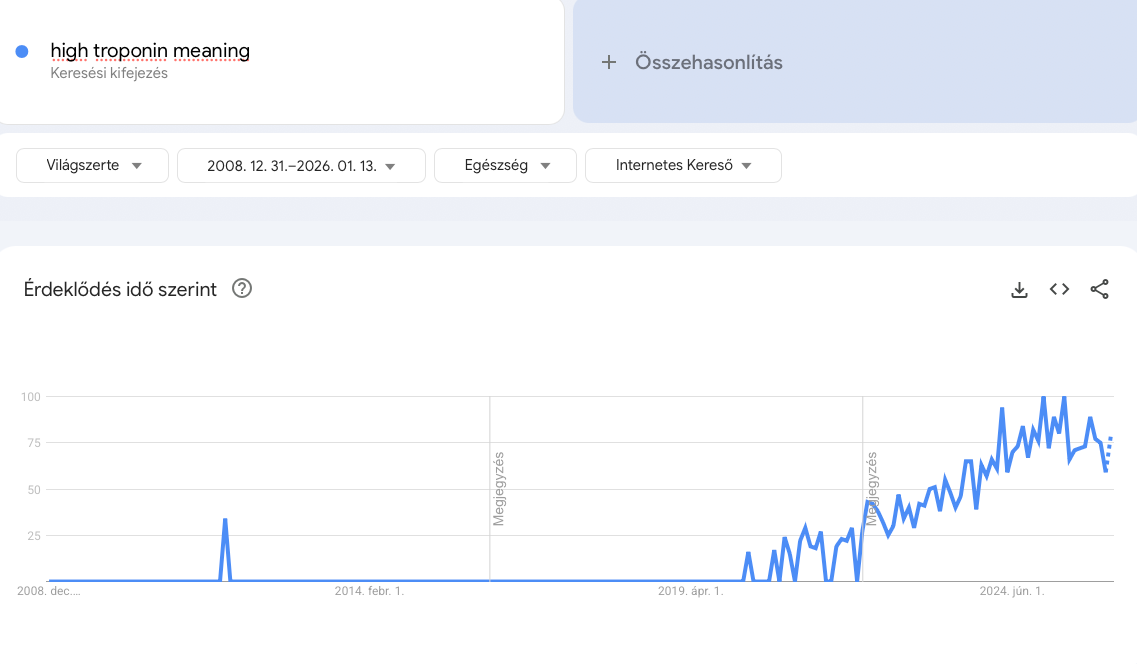
The cry for help of the heart muscle. Troponin is a protein that enters the bloodstream only when heart muscle cells die. The dramatic rise of the graph starting in 2021 does not merely indicate “heart problems,” but shows that the heart muscle of large populations has suffered irreversible damage. The 2024 peak of the curve proves that the process has not stopped — myocarditis and cardiac damage have become chronic within society.
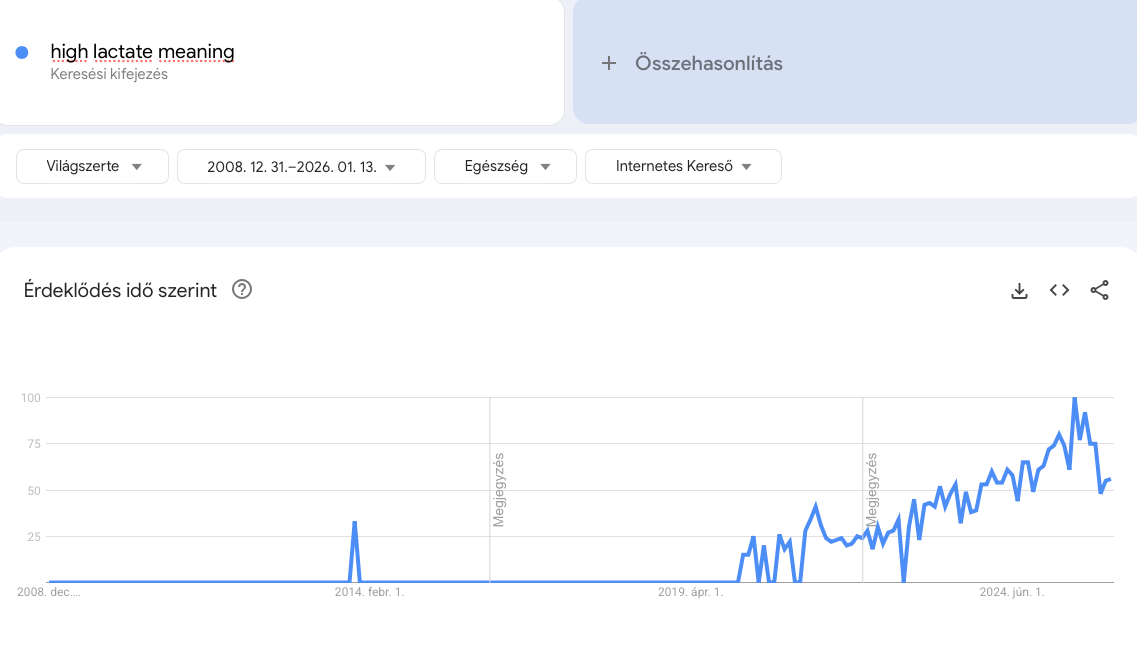
Cellular-level suffocation. Elevated lactate levels are not merely the “muscle soreness” of athletes. At rest, they indicate tissue oxygen deprivation (hypoxia). When capillaries are blocked by microclots (see: Microclots), cells do not receive oxygen and are forced to switch to emergency mode. This graph explains the crippling, leaden fatigue experienced in “Long COVID” and among the vaccine-injured: their bodies are literally suffocating, even as they continue to breathe.
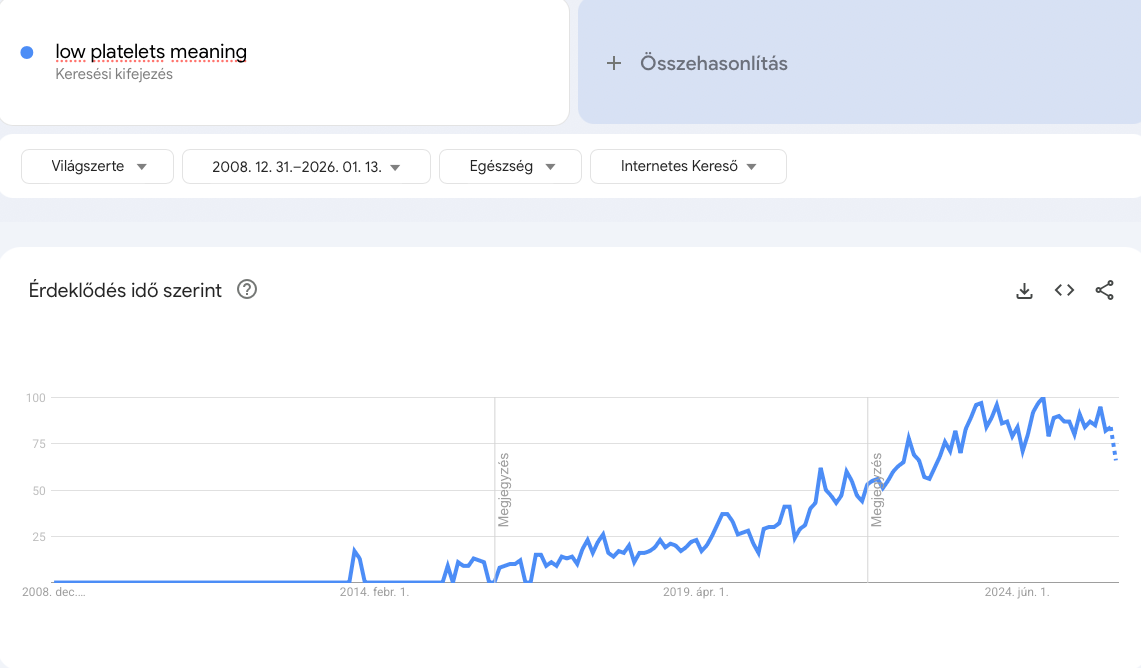
Where do the platelets go? A low platelet count most commonly occurs when the body “uses them up” somewhere. This graph is evidence of silent coagulation disorders: the countless microscopic clotting processes taking place within the body (micro-clotting) consume platelets, leading to bleeding tendency and, paradoxically, to an increased risk of thrombosis.
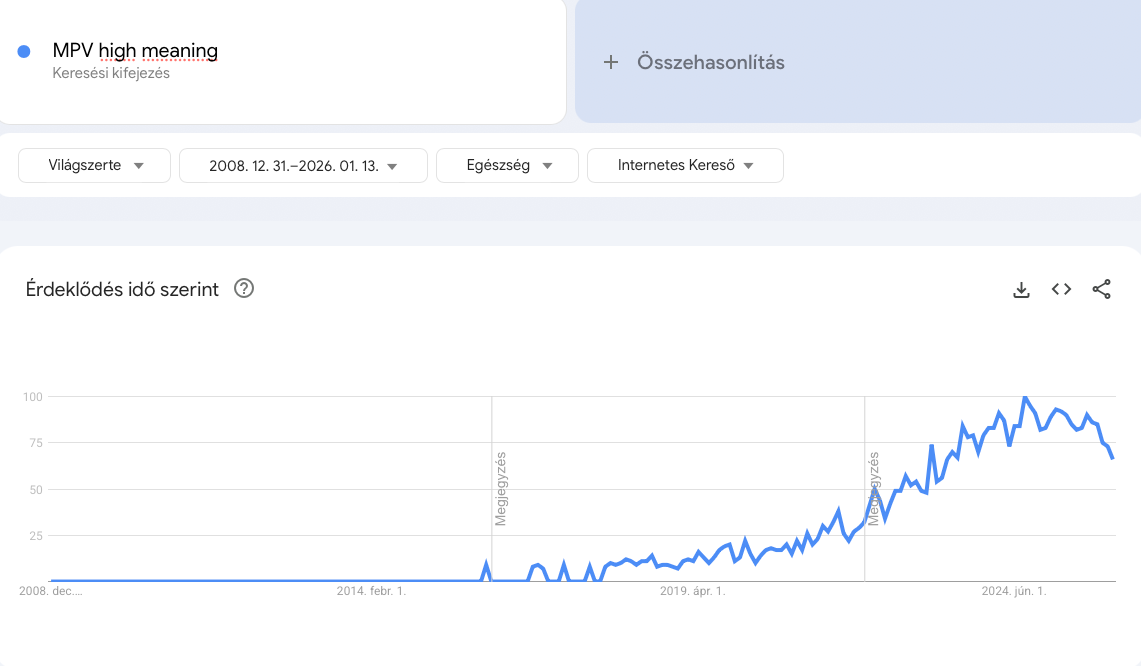
The coagulation system in panic. An increase in MPV (Mean Platelet Volume) indicates that the bone marrow is desperately trying to produce new platelets, because the older ones have been depleted (see the graph above). However, larger, “younger” platelets are more aggressive and more prone to clot formation. This trend indicates a growing, structural predisposition to thrombosis across the population.
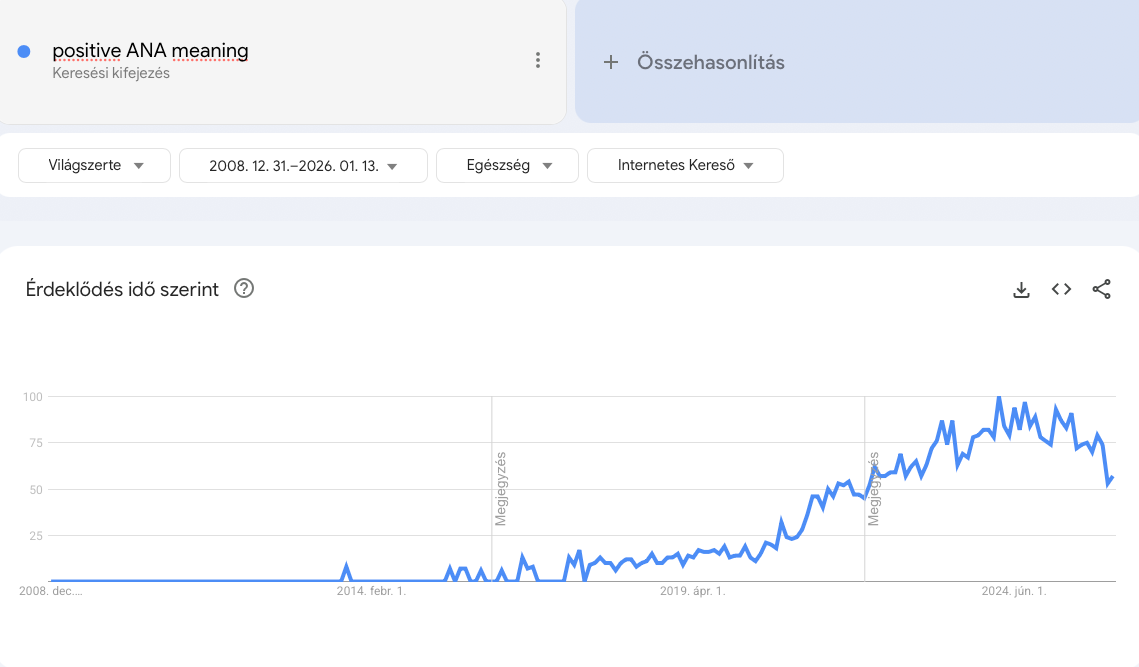
Civil war within the body. Rising ANA levels are a classic sign of autoimmunity: the immune system no longer recognizes the body’s own cells and attacks them as enemies. The steep trajectory of the graph suggests that, as a result of interventions, the immune systems of millions have been misprogrammed, leading to chronic inflammation, fatigue, and an explosive spread of autoimmune conditions.
So if we set propaganda aside and look at what the population of the Western world searches for in desperation in the middle of the night, this horrifying pattern emerges.
These graphs do not lie. They show that millions of people are receiving laboratory results they do not understand, and to which their doctors respond with a shrug: “It’s probably just stress.” But people feel that something is wrong. They are experiencing firsthand what official statistics conceal.
To witness this chasm between reality and the official narrative…
well, that is what truly consumes and exhausts a person.
So when I saw the video below, I realized that nothing describes the struggle of the past years more perfectly than this. This is how I feel somewhere inside, and perhaps how many of us feel who try to fight the tsunami of global brainwashing with facts, data, and rationality.
After all, in recent years I have invested a tremendous amount of energy into presenting the most painful topics in a way that is as understandable as possible, while still maintaining proper professional rigor. I have written about the suppressed risks of the childhood vaccination schedule, the biological traps of mRNA technology during the COVID period and the gigantic industrial interests operating in the background, as well as about substances that could have saved millions of lives or significantly improved their condition.
Just a few pieces from the recent period:






But the point is not my work, rather that experts, physicians, and researchers with far greater knowledge than minehave proven the truth again and again, in black and white.
And what happened?
The rain keeps falling, the water keeps pouring through the open gate,
and the crowd drifts with the current.
And we stand there with our bucket, shoveling. At times like this, a person sometimes puts the shovel down and asks the question: does this have any meaning at all?
It may seem that a large part of humanity is unable — or unwilling — to recognize the truth, for example when it comes to vaccines entangled in complex, multi-actor, multi-billion-dollar interests. The noise is too loud, the money is too great, the scientific indoctrination too deep.
So now I am stepping back to the basics. To the most primitive, simplest level.
I will not be writing about genetic engineering or virology,
but about a piece of fabric. The mask.
Because if society is unable to scientifically discard this “wretched” device — which anyone with common sense and basic knowledge of physics can see does not work in the way it is claimed — if, in this elementary physical question, dogma prevails over reality, then how could we possibly expect change in matters that threaten far greater financial interests?
The mask may therefore be the litmus test. If we fail here, we fail at everything. But if we are able to see — or help others see — reality at this point, then perhaps there is hope for the rest as well.
So I pick up the shovel again — only this time, I start with a smaller puddle.

The Illusion of the Protective Shield: When science once again hardens into dogma
One of the greatest paradoxes of modern medicine is not what we do not know, but what we believe we know yet are wrong about — or worse still, when we already know something but choose to ignore it, so as not to admit that we were complicit in spreading falsehoods. The history of masks is not merely a medical-historical curiosity, but a precise social diagnostic: it shows how ritual can override evidence, and how false reassurance becomes the enemy of real protection.
When we enter an operating room — whether physically or through the frames of a television series — the image is iconic: sterile lights, soft beeping, and the unavoidable masks on physicians’ faces. This image is the “sanctity” of modern medicine. It conveys the message: science reigns here, there is no room for chance, everything serves the fight against infection.
But what if this image is merely theater? What if the mask in the operating room protects not the patient from infection, but rather the physician and the institution from accountability? And most importantly: what does this say about us, about a society that places blind trust in solutions that merely appear scientific?
The zero-level assumption
It seems logical: the human mouth contains bacteria, the surgical wound must be sterile, therefore we place a barrier between the two. This is mechanical thinking. Biological reality, however, is rarely this linear.
To understand the nature of dogma, we must examine outcome-based evidence. Not what we think about how masks should work, but what statistics actually show about their use.
What the studies actually found
In the second half of the 20th century, when evidence-based medicine (EBM) began to gain ground, there were, naturally, researchers who asked the heretical question:
Does wearing a mask actually lead to fewer infections?
The results were shocking — and unfortunately they still are today, as nothing has changed. At the end of the article, many more studies are cited; here are just a few:
The Tunevall Study (1991): Dr. T. G. Tunevall, a Swedish surgeon, conducted a radical experiment. Over a 115-week period, 3,088 surgical procedures were performed. Surgeons were randomly assigned either to wear masks or not.
The result: In the masked group, the infection rate was 4.7%. In the non-masked group? 3.5%. Although the difference was not statistically significant, the trend clearly did not favor mask use.The Orr Observation (1981): Dr. Orr had already concluded earlier that wearing a mask not only fails to reduce infections, but in certain cases may increase them. His explanation was mechanical: small adjustments made while wearing the mask, friction of the mask against the face, and forced airflow can increase the dispersal of skin flora(bacteria-laden epithelial cells).
The Cochrane analysis verdict (2016): The Cochrane Library, often considered the “supreme court” of medical evidence, reviewed all available relevant studies. Their conclusion was sobering:
“We found no statistically significant difference in infection rates between masked and unmasked groups.”Then the updated Cochrane Review (Jefferson et al., 2023):
The comprehensive 2023 review titled “Physical interventions to interrupt or reduce the spread of respiratory viruses” is not just one study among many. Cochrane Reviews represent the gold standard of medical science: they systematically collect and synthesize the highest-quality evidence under strict protocols, excluding weak or biased studies.
Are masks completely ineffective against the spread of COVID and influenza? (Yes, they are.)
The findings were unacceptable to the mainstream: according to the authors, there is no high-quality evidence that any mask reduces the community spread of respiratory viruses.
Medical masks: The researchers included 12 large-scale studies in their analysis. The conclusion: community mask use probably makes little or no difference in the outcomes of influenza-like and COVID-19–like illness compared with not wearing masks.
N95 / FFP2 masks: The experts also examined the effectiveness of the supposedly “safer” N95/P2 masks compared with medical masks. The result was again sobering: for laboratory-confirmed influenza and COVID-19, there is probably no difference in protective effect between medical masks and N95/P2 masks in community settings.
The researchers also made another critically important — and highly relevant — observation: the harms of mask-wearing were rarely reported in the reviewed studies, or the reporting was of poor quality. Thus, science has not only failed to confirm effectiveness, but has also failed to adequately assess the risks.
If this were a drug — and of course if it were not already known that authorities serve certain interests — it would never be approved, because it has no proven benefit, yet carries potential harm.
Let us make the invisible visible
It is often said, “I’ll believe it when I see it.” Yet the microscopic world of viruses and bacteria is invisible to the human eye, and it is precisely this invisibility that allows myths and false senses of security to take hold. But what happens if we make the air we inhale and exhale visible?

In the videos below, we can see simple yet highly illustrative physical demonstrations. Using an electronic cigarette, breathing through masks becomes visible: the dense white vapor consists of aerosol particles that behave physically in a similar way to exhaled, potentially infectious breath.
These recordings are not laboratory theories, but raw reality.
What we see is a shockingly simple refutation of the theory of the “mask as a protective barrier.” Regardless of the type of mask, the videos show with crystal clarity that air — and with it, particles — finds its way through.
The laws of physics cannot be suspended by decrees. If the mask material truly blocked everything, the wearer would suffocate within seconds. But because we must be able to breathe, the exhaled “cloud” flows freely through the pores of the fabric, or escapes uncontrollably around the nose bridge and through the side gaps.
This demonstration exposes the greatest lie of enclosed spaces (offices, shops, elevators): in a closed room, the amount of pathogens released into the air is exactly the same with a mask as without one.
At most, the mask changes the direction of airflow, but it does not reduce the emitted “load.” Smoke does not lie — and as we see in the videos, the illusion of protection dissolves within moments in the swirling vapor.
Let us go further and examine how this “protection” can actually be harmful.
If the mask does not function as a physical wall, then how does it function? This is where aerosol physics and microbiology come into play — disciplines that dogma often ignores.
The “Venturi effect” in practice: The mask does not form a hermetic seal. When the wearer exhales, the air does not disappear; instead, it accelerates and escapes sideways and upward — often toward the eyebrows, from where shedding epithelial cells may fall into the surgical field. This deflection of airflow can paradoxically cause more targeted contamination than slow, unobstructed exhalation.
The Petri-dish effect: Under the mask, a warm, humid microclimate develops. This is an ideal incubator for bacteria. During long surgical procedures, the mask becomes damp, and the filter turns into a “capillary bridge” through which microorganisms can easily migrate.
The psychological trap: the theater of safety
Why, then, do we cling to it so desperately? The answer lies not in virology, but in psychology.
This is risk compensation (also known as the Peltzman effect). When people feel protected, they tend to behave more riskily. The mask functions as a psychological “armor.” A surgeon wearing a mask may, at a subconscious level, speak more freely over the wound and pay less attention to maintaining distance, because the problem feels “taken care of.”
In reality, the vast majority of surgical infections do not originate from the air (breath), but from contact (hands, instruments, skin). The mask, however, diverts attention from these critical points.
Social diagnosis: Why are we afraid of facts?
The case of surgical masks is a perfect model of how our society functions today. We see an intervention that:
Intuitively seems correct (“better safe than sorry”).
Is visually striking (it immediately distinguishes “responsible” behavior from “irresponsible”).
Is not scientifically proven to deliver the expected effectiveness.
Yet if someone attempts to abandon it, they are labeled not an innovator, but a heretic. Why?
Because the mask (in this context) has crossed from the category of a functional tool into that of a liturgical object. Both in medicine and in societal governance, there exists “institutional self-protection.” For a hospital administrator, the mask does not serve to protect the patient, but to avoid legal liability.
“We did everything, we followed the protocol,” they say — even when the protocol is outdated, or even harmful. Sadly, this applies to so many other things as well in our increasingly sick world, driven from above by protocols.
This phenomenon highlights a dangerous tendency: we are inclined to accept interventions that disguise themselves as healing, but in reality provide only the illusion of control. Whether we are talking about public health measures, economic austerity, or educational reforms, we often forget to measure outcomes, because intent (“we wanted to help”) blinds us to the result (“we did not help — we even caused harm”).
The bastard offspring of protocol: when hygiene turns into a breeding ground for bacteria
If the effectiveness of mask use in the operating room is debatable, then forcing it on the general population was a direct mockery of medical rationality. In surgery, there is a strict, iron rule that was conveniently “forgotten” during the social experiment: sterility and time limits.
A surgeon puts on a mask once. If a procedure is prolonged, the mask must be replaced as soon as it becomes damp(after roughly 2 hours). At the end of use, it is immediately disposed of as hazardous waste.
By contrast, what happened in society?
The population was forced to use a single-use device — without any scientific justification. A mask crumpled in a pocket, hung on a car’s rear-view mirror, or thrown onto a table is a microbiologist’s nightmare.
The “pocket incubator”: Inside a used mask, exhaled moisture, saliva, and environmental dust form a perfect growth medium. Stored in a pocket near body temperature, the fabric turns into a breeding ground for bacteria and fungi. When a person places this contaminated material back in front of their face and takes a deep breath, they are not inhaling fresh air, but delivering concentrated pathogens directly into their lungs. This practice did not curb the epidemic — it dramatically increased the risk of bacterial pneumonia and secondary upper respiratory infections.
A valóság a mikroszkóp alatt: Amikor a maszk visszatámad
Sokan felteszik a kérdést: “Mi baj lehet abból, ha hordom? Legfeljebb nem használ.” A következő demonstráció azonban megmutatja, hogy a válasz ennél sokkal riasztóbb. A “nem használ” és a “aktívan árt” között óriási a különbség.
Egy egyszerű házi kísérletben – amelyet egy mikrobiológiai laboratóriumban elemeztek ki – megnézték, mi tenyészik ki a különböző állapotú maszkokból, ha táptalajra (véragarra) helyezik őket.
A videóban látható esetek nem extrém kivételek, hanem a mindennapjaink tükörképei: a táska mélyén lapuló “tartalék”, a kórusban átizzadt textil, és a sokak által gyakorolt “takarékos” megoldás, a hetekig hordott eldobható maszk.
Az eredmények önmagukért beszélnek. Ami a Petri-csészében “kivirágzik” – a Staphylococcustól a Streptococcuson át a gombákig –, az pontosan az a koktél, amit a maszk viselője minden egyes lélegzetvétellel újra és újra visszainhalál a tüdejébe. Külön figyelmet érdemel a videó végén látható “5-ös számú minta” (a 3 hetes maszk): ez már nem védőeszköz, hanem egy komplett biológiai veszélyforrás.
Íme a bizonyíték arra, hogy a “zseb-inkubátor” nem csak elmélet:
The mask as a psychological weapon
There is, however, another function of the mask — even more insidious than biological contamination — about which the mainstream of science remains deeply silent: the connection between psychological conditioning and immune suppression.

Mandating mask use was not merely a public health measure, but a visual perpetuation of a state of emergency.
The mask became a giant billboard fixed to the face, constantly screaming:
“You are in danger! You are sick! The other person is a threat!”
This continuously maintained fear-mongering is not a harmless inconvenience, but a biological attack on the body:
Chronic stress response: Constant fear and a persistent “illness awareness” (the belief that anyone, at any time, may be infectious) raise cortisol levels.
Immune suppression: Sustained elevated cortisol is proven to inhibit immune function and reduce lymphocyte counts.
The self-fulfilling prophecy of fear: Psychoneuroimmunology has long established that those who fear illness become more susceptible to it.
By forcing society behind masks, a mass psychosis was generated. Covering the face dehumanizes, cuts off social connection (one of the immune system’s key supports), and pushes individuals into an isolated, anxious state. This intervention was particularly devastating for those who were already afraid of viruses: for them, the mask did not provide protection, but cemented panic, making them biologically more vulnerable to real infections.
The silenced solution:
Nasal breathing and the body’s internal chemical shield
While news broadcasts and posters relentlessly drilled into people that a piece of fabric was the only thing that could protect us, they remained deeply silent about the real “superweapon.” This weapon is not found on pharmacy shelves, but in the middle of our face: the nose.
One of the great failures of modern medicine — among many — was that during the pandemic, attention was not drawn to the importance of nasal breathing. In fact, mandatory mask use produced the opposite effect. The mask creates breathing resistance (making it harder to inhale), which causes people to involuntarily switch to mouth breathing in order to obtain more oxygen.
By doing so, they disable the body’s primary built-in antiviral defense system.
Nitric oxide (NO): nature’s disinfectant
Why is breathing through the mouth a problem? Because the mouth is merely a “tube” that delivers cold, dry, unfiltered air (and the pathogens it contains) directly into the lungs. The nose, by contrast, is a complex filtering and gas-mixing system.
In 1998, three scientists (Furchgott, Ignarro, and Murad) were awarded the Nobel Prize in Medicine for discovering the physiological effects of nitric oxide (NO). It was shown that this gas is continuously produced in the paranasal sinuses and mixes with inhaled air during nasal breathing.
Nitric oxide has two critical effects:
Vasodilatory effect: It improves pulmonary blood circulation, allowing 10–20% more oxygen to be utilized from air inhaled through the nose compared to mouth breathing.
Powerful antimicrobial effect: NO is a strong oxidizing agent. Viruses — which are genetic codes enclosed in simple protein shells — are extremely sensitive to oxidative stress.
Here, too, the science is clear.
Studies have confirmed (including during the 2005 SARS outbreak) that nitric oxide inhibits viral replication and directly damages viruses. Viruses are far more vulnerable to this oxidative effect than bacteria (which have their own metabolism and more resilient cell walls), although high concentrations of NO are capable of neutralizing bacteria as well.
The mask paradox
When a person puts on a mask and, due to increased breathing resistance, opens their mouth, the following happens:
Bypassing the filter: Air no longer passes through the nose’s cilia and mucous membranes.
Bypassing disinfection: The air is no longer enriched with virus-killing nitric oxide.
Direct route to the lungs: Pathogens reach the lower airways unimpeded.
Thus, wearing a so-called “protective device” paradoxically inhibits the very mechanism — nasal breathing — that would provide the most reliable defense against respiratory viruses.
If the goal had truly been public health, shopping centers should not have instructed people to wear masks, but to keep their mouths closed and breathe consciously through their noses. This is the only intervention that is free, has no side effects, and has been shown to reduce the severity of infections.
Practical advice: “humming” as an internal turbocharger
Few people know that the effectiveness of this natural defense can be multiplied by a simple, scientifically validatedmethod.
Soft humming with a closed mouth — a prolonged “mmm” sound during exhalation — creates subtle vibrations in the paranasal sinuses. This physical oscillation “ventilates” the sinuses and increases nitric oxide release by orders of magnitude. According to measurements from the Karolinska Institute, nasal NO concentrations during humming can rise to up to 15 times higher than during quiet nasal breathing. https://www.atsjournals.org/doi/full/10.1164/rccm.200202-138BC
This small, conscious practice (just a few minutes a day, while walking or resting):
dramatically boosts the production of the body’s own “internal disinfectant” gas,
improves lung oxygenation,
and does all of this without side effects, devices, or external coercion.
Imitating nature: the external oxidative shield and censored solutions
There is a striking connection that few people notice. We have just seen that the body’s own internal line of defense(nitric oxide) is an oxidative gas that destroys invaders through chemical reactions.
This raises the question: if nature has chosen this mechanism as the most effective form of protection, can we apply something similar from the outside, assisting the body’s work?
The answer is yes. There exists another gas whose mechanism of action is eerily similar to that of nitric oxide. This gas is chlorine dioxide (ClO₂).
Because I have been working in this field for years and am very familiar with its mechanism of action, in 2020, at the beginning of the COVID hysteria, before vaccines, I felt it was my duty to share this knowledge. Not “internet wisdom,” but a joint study by professors of the Budapest University of Technology and Economics and Semmelweis University (Dr. Zoltán Noszticzius and colleagues), published also in English.

The result? “Big Brother” struck immediately.
I received an instant ban on Facebook.
Algorithms and “fact-checkers” deemed the Hungarian research — which could have saved thousands of lives — to be dangerous, while unscientific mask-wearing was made mandatory.
Why were they afraid of this information?
Because chlorine dioxide (in aqueous solution) is an extremely “intelligent,” selective oxidizing agent. Many people — either mistakenly or through deliberate misrepresentation — confuse it with bleach (sodium hypochlorite). This is a serious error.
Bleach causes indiscriminate damage, leaves behind toxic chlorine byproducts, and does not differentiate: it kills pathogens and human cells alike.
Chlorine dioxide, however — much like the body’s own nitric oxide — is size-selective.
The “chemical scissors” that cut the virus
Hungarian researchers identified the core mechanism: the “spikes” on the surface of viruses (which they use to bind to our cells) are rich in certain amino acids (cysteine, tyrosine, tryptophan) that are extremely sensitive to oxidation.
When we gargle or use a nasal spray, chlorine dioxide oxidizes these amino acids within fractions of a second. It effectively burns off the virus’s key. Without the key, the virus cannot enter the cell, and therefore cannot replicate.
And most importantly: because we humans are multicellular giants compared to viruses, and our cells are protected by robust antioxidant defenses, this oxidative effect is harmless to us. Our bodies recognize this mechanism, since — as we have seen — they use the same strategy in the nasal sinuses.
The missed open goal
The formula could have been remarkably simple:
Internal defense: Nasal breathing and “humming” (nitric oxide production).
External support: Regular gargling and nasal spray (chlorine dioxide).
With these two oxidation-based methods, viral load in the throat and nasal cavity could have been dramatically reduced, preventing pathogens from reaching the lungs in large numbers.
Instead, we were given a dirty piece of fabric — and censorship.
This, we were told, was “following the science.”
For further, in-depth information on chlorine dioxide, you can click HERE.
We cannot avoid the obvious conclusion. Why did every alternative have to be eradicated with fire and sword? The answer lies in legal regulation.
Everything revolved around forcing through experimental, gene-technology–based mRNA vaccines that lacked adequate long-term studies. These products, however, could enter the market only through the loophole of the “Emergency Use Authorization” (EUA).
But this authorization has a strict, non-negotiable condition: it may be issued only if there is no other available and effective treatment for the disease.
Seen in this light, censorship suddenly makes sense. Had authorities acknowledged that chlorine dioxide (CDS), ivermectin, or other cheap and effective treatments worked, the legal foundation of the mRNA vaccines — and the multi-billion-dollar business behind them — would have collapsed like a house of cards. This is how these solutions — and with them, very likely thousands of human lives — became casualties of the “vaccine agenda.”
Back to common sense
The history of surgical masks, the ignoring of scientific data, the immunosuppressive effects of fear, and the suppression of basic physiology (nasal breathing) all point in the same direction.
The system that should be responsible for our health once again steered society into the labyrinth of false protocols, and instead of true healing and prevention, it chose measures that lead to illness.
The lesson is bitter, yet liberating: the key to our health lies not in external coercive tools, but in understanding and supporting the functioning of our own bodies.
It is time to take off the mask — both metaphorically and literally — to close our mouths, and to take a deep breath through our noses. Because clean air and clear thinking are the best immune boosters.
Closing thought
Science should not be a collection of dogmas, but a methodology that allows us to recognize and correct our mistakes. When data have demonstrated for decades that a tool does not deliver the results attributed to it, yet we still cling to it, we have left the realm of science and entered the world of belief and dogma.
If we are unable to let go of the dogma of such a simple, primitive tool as the mask, even when contradictory data have been available for decades, what chance is there that we will ever honestly re-examine far more complex and consequential health dogmas?
Is there a realistic chance that health itself will one day truly become the primary consideration, rather than protocols, rule systems, and “untouchable truths” shaped by pharmaceutical or other industrial interests?
We must acknowledge that modern “healthcare” in many cases is no longer about healing, but about maintaining the system behind it.
One thing, however, is certain: no one can evade individual responsibility. When we uncritically accept or uphold performative measures that are already known not to serve our health, we — consciously or unconsciously — become participants in the theater of false security ourselves.
The blacklist of scientific evidence
What the scientific literature actually says about the effectiveness of masks
A common argument is that mask effectiveness represents a “scientific consensus.” The list below — consisting of studies published in peer-reviewed medical journals — demonstrates that the consensus points in precisely the opposite direction. If masks are unable to stop bacteria in a sterile operating room (organisms that are orders of magnitude larger than viruses), then expectations regarding viral protection are nothing more than wishful thinking.
The refutation of masks: bacterial and surgical wound infection studies
These studies demonstrate that mask use in operating rooms did not reduce, and in some cases even increased, infection rates.
1. Orr, N. W. (1981): Fewer masks, fewer infections
Dr. Orr’s surgical team did not wear masks for six months. The result was striking: the rate of surgical wound infections decreased significantly compared to the period when masks were worn.
Conclusion: “The wearing of a mask is a standard procedure that could be abandoned.”
Source: Annals of the Royal College of Surgeons of England (Link)
2. Tunevall, T. G. (1991): The great Swedish experiment
A general surgical team performed 3,088 operations over two years. Among those wearing masks, the infection rate was 4.7%, while in the non-masked group it was only 3.5%.
Source: World Journal of Surgery (Link)
3. Cochrane Review (2016): The highest level of evidence
The comprehensive analysis authored by Vincent and Edwards, updated in 2016, reached the following conclusion: “No statistically significant difference in infection rates was found between masked and unmasked groups in any of the studies.”
Source: Cochrane Database of Systematic Reviews (Link)
4. The Karolinska Institute decision (2010)
Anesthesiologists at the institute responsible for awarding the Nobel Prize abolished mandatory mask use. Dr. Eva Sellden’s justification was clear: “There is no evidence to support this practice.”
Source: Anesthesiology (Link)
5. Webster et al. (2010): Obstetrics and gynecology
In a study involving 827 patients, the infection rate was 11.5% in the masked group, compared to 9.0% in the non-masked group.
Source: ANZ Journal of Surgery (Link)
Additional relevant studies:
Ritter et al. (1975): Mask use did not reduce contamination in the operating room. (Link)
Ha’eri & Wiley (1980): Using a microsphere experiment, they demonstrated that particles originating from the mask entered the surgical wound in every case. (Link)
Laslett & Sabin (1989): During cardiac catheterization, omission of mask use did not result in infections. (Link)
Skinner & Sutton (2001): The available evidence supports discontinuing mask use. (Link)
Lahme et al. (2001): Masks were found to be unnecessary during regional anesthesia.(Link)
Carøe (2014): A review of 6,006 patients found no difference. (Link)
Salassa & Swiontkowski (2014): There is no evidence that masks reduce infection rates. (Link)
Da Zhou et al. (2015): There is a lack of evidence that masks protect either the patient or the surgeon. (Link)
The virus reality: respiratory viruses and COVID-19 studies
If the studies above addressed bacteria, what does science say specifically about viruses and the pandemic? The answer is the same.
1. The DANMASK-19 Study (Bundgaard et al., 2020)
This was the world’s first large randomized controlled trial (RCT) specifically examining the relationship between community mask use and COVID-19 transmission. It was conducted in Denmark with more than 6,000 participants.
Result: There was no statistically significant difference in SARS-CoV-2 infection rates between the mask-wearing group and the control group. The mask provided no measurable protection to the wearer.
Source: Annals of Internal Medicine (Link)
2. The updated Cochrane Review (Jefferson et al., 2023)
Physical interventions to interrupt or reduce the spread of respiratory viruses.
This comprehensive analysis, considered the “gold standard” of medical evidence, concluded that community mask use — whether medical masks or N95-type masks — probably makes little or no difference in reducing the spread of respiratory viruses (influenza, COVID-19) compared with not wearing masks.
Source: Cochrane Library (Link)
Additional referenced literature and sources:
Tunevall T.G. (1991). Postoperative wound infections and surgical face masks: A controlled study. World Journal of Surgery.
The study showed that abandoning mask use did not increase infection rates.
Link (PubMed)Orr N.W. (1981). Is a mask necessary in the operating theatre? Annals of the Royal College of Surgeons of England.
An early study that suggested that mask use may increase bacterial contamination in the surgical field.
Link (PMC)Vincent, M., Edwards, P. (2016). Disposable surgical face masks for preventing surgical wound infection in clean surgery. Cochrane Database of Systematic Reviews.
A comprehensive meta-analysis that found no significant evidence of a protective effect of masks in clean surgical procedures.
LinkThe Nobel Prize in Physiology or Medicine 1998.
LinkThe antiviral effect of nitric oxide (NO) (SARS-CoV study):
Åkerström, S., et al. (2005). Nitric Oxide Inhibits the Replication Cycle of Severe Acute Respiratory Syndrome Coronavirus. Journal of Virology.
This study specifically demonstrated that nitric oxide (NO) inhibits coronavirus replication.
Link (PubMed)Lundberg, J.O.N. (2008). Nitric oxide and the paranasal sinuses. The Anatomical Record.
A detailed description of how nitric oxide (NO) is produced in the paranasal sinuses and how it sterilizes inhaled air.
LinkWeitzberg, E., Lundberg, J.O.N. (2002). Humming Greatly Increases Nasal Nitric Oxide. American Journal of Respiratory and Critical Care Medicine. Link