Hidden Behind the Common Good: The Real Risks of Vaccination Technologies and the Delusion of Herd Immunity
HUNGARIAN: A közjó mögé bújtatva: Az oltási technológiák valós kockázatai és a nyájimmunitás téveszméje
MAGYAR VERZIÓ IDE KATTINTVA OLVASHATÓ.
Where the risk is personal, the freedom of choice must be as well – especially when it lasts a lifetime…
The debate surrounding mandatory vaccinations is often reduced to an oversimplified battle: a clash between individual freedoms and the collective good. This essay attempts to look behind that false dilemma. Because what happens if the sacred banner of the “common good” hides technologies and assumptions whose built-in risks and errors have never truly been weighed?
The official narrative wears the armor of unquestionable science, yet in reality it defends a system where doubt is suppressed. And where questioning becomes a sin, science ceases to serve understanding and becomes the servant of dogma. This summary therefore does not seek to judge, but rather serves as an honest appeal to those who have so far taken what they heard at face value – as most of us once did. This call merely asks for sincere attention, openness, and courage so that we may think together and dare to broaden our knowledge.
Let us read, ask, and dare to doubt. True science begins here. And our responsibility for the health of our children cannot end with a doctrine.
And if uncertainty in this matter is indeed real, coercion can never be the answer.
In the above video, Professor Bret Weinstein, evolutionary biologist, summarized the situation briefly and sharply:
None of the three fundamental vaccination technologies can be considered inherently safe:
1. The first, the live attenuated virus technology, is risky because the human body reacts to it individually. What causes a mild, harmless infection in one person may trigger a severe illness in another. Even more importantly, the virus can mutate and regain its virulence, as evidenced by the numerous cases of vaccine-derived poliomyelitis.
This technology teaches the immune system to defend itself through a mild, controlled infection. Examples include the measles–mumps–rubella (MMR) vaccine or the orally administered poliovirus vaccine.
The built-in flaw: genetic instability
Viruses mutate extremely rapidly. The attenuated virus begins to replicate within the vaccinated person’s body, and during this process of mutation it can “relearn” the very traits that make it dangerous. This phenomenon is not theoretical. The World Health Organization (WHO) documents outbreaks of vaccine-derived poliomyelitis. These are not caused by the “wild” virus, but by the virus contained in the vaccine, which, circulating within a vaccinated individual or the community, regains its virulence. Studies published in The Journal of Infectious Diseases confirm that attenuated vaccine strains can genetically revert, turning a preventive tool into the very source of an outbreak.
Famulare (2015) – Sabin Vaccine Reversion in the Field
The study showed that live attenuated poliovirus vaccines (OPV) can undergo genetic reversion within vaccinated individuals and potentially regain wild-type virulence.
🔗 Journal of Virology, 2015
Gray et al. (2023) – The Origins and Risk Factors for Serotype-2 Vaccine-Derived Poliovirus
According to the research, strains derived from the OPV2 vaccine can revert to forms that cause neurovirulence, and through transmission, they can initiate new vaccine-derived poliovirus outbreaks.
🔗 The Journal of Infectious Diseases, 2023
CDC/WHO (2024) – Circulating Vaccine-Derived Poliovirus Outbreaks, 2023–2024
According to data from the WHO and the CDC, between 2023 and 2024 a total of 74 vaccine-derived poliovirus (cVDPV) outbreaks occurred across 39 countries, confirming that the phenomenon is not theoretical but a real public health problem.
🔗 MMWR Weekly Report, CDC, 2024
2. The second method, using an inactivated virus or its fragments, is too weak on its own and therefore requires a chemical booster called an “adjuvant” to trigger a panic reaction in the immune system. The problem? This immunological alarm is non-specific. The immune system may attack not only the vaccine’s intended target but also random substances — such as pollens or even the body’s own tissues — thus paving the way for allergies and autoimmune diseases.
This technology appears safer: here the virus is completely killed, or only a fragment of it is used, so it cannot replicate or mutate. The problem is that the immune system does not consider a dead pathogen or one of its fragments a serious threat and would not mount a strong response to it. To make it work, a chemical booster called an “adjuvant” is added to the vaccine. The most common of these substances is aluminum. The adjuvant’s role is to sound a general, non-specific alarm — a kind of immunological “fire drill” — within the body.
The built-in flaw: uncontrolled immune panic and its two fatal consequences
The adjuvant does not tell the immune system “attention, here is the measles antigen,” but rather shouts “PANIC! WE ARE UNDER ATTACK!” In the ensuing confusion, the immune system in this heightened alert state can commit three fundamental and catastrophic errors: it can attack harmless external substances, the body’s own healthy tissues, or — even worse — the adjuvant itself may become a slow-acting toxin in our most sensitive organ.
Consequence: The allergy epidemic – misidentification of the external enemy
The scientific mechanism is the disruption of the Th1/Th2 balance. The immune system has a “commando unit” (the Th1 response) effective against intracellular pathogens, and an “air force” (the Th2 response), which is also responsible for allergic reactions. Aluminum adjuvants have been scientifically proven to strongly shift the immune system toward the Th2 response (the allergic tendency). The process is tragically simple: if the immune system, in its state of panic, encounters a harmless allergen (such as food or pollen), it labels it as an enemy as well, creating a lifelong allergy.
Robert F. Kennedy Jr., the current U.S. Secretary of Health, stated in the interview that in laboratory experiments, aluminum adjuvants are used to induce persistent allergies in animals — and the same adjuvants are present in human vaccines. He refers to researchers Mawson and Cowlings, who argue that environmental antigens present at the time of vaccination — such as pollens — can trigger lifelong allergies. According to Kennedy, the NIH is currently investigating whether these aluminum adjuvants may be linked to the allergy epidemic that began in 1989, coinciding with the expansion of the American vaccination schedule.
Consequence: Autoimmune diseases – creating the internal enemy
There is a darker side to this panic. In the chaos, the immune system may not only target harmless external substances but also mistake the body’s own healthy tissues for enemies. Through mechanisms such as molecular mimicry (when vaccine proteins resemble the body’s own building blocks) or bystander activation (when self-cell debris becomes suspicious in an inflamed environment), the immune system can turn against itself. This can lead to chronic diseases such as multiple sclerosis, rheumatoid arthritis, type 1 diabetes, or inflammatory bowel diseases.
Consequence: Silent inflammation of the brain – the neurotoxic Trojan horse
There is a third, perhaps most alarming consequence of uncontrolled panic, related to the physical path of the adjuvant. Aluminum was long believed to remain at the injection site and gradually be eliminated. However, modern research has shown that this is not true. The injected aluminum particles are engulfed by the immune system’s cleanup cells — macrophages. Yet these cells are not stationary; they travel throughout the body and are capable of crossing even the most tightly guarded barrier — the blood-brain barrier.
This is the Trojan horse mechanism: the immune cell, whose task would be to neutralize the toxin, becomes the very vehicle that delivers it into the central nervous system. In the brain, aluminum behaves as a biopersistent (hard-to-degrade), highly neurotoxic substance. Its presence triggers chronic inflammation (neuroinflammation), continuously activating the brain’s own immune cells, the microglia. This persistent, low-level inflammatory state in a developing child’s brain can have catastrophic consequences, contributing to cognitive and behavioral disorders, learning difficulties, and neurodegenerative processes.
The price of this technology’s effectiveness, therefore, is an uncontrolled immunological panic — during which the body may learn to attack peanuts, ragweed, its own nervous system, or even allow a neurotoxin to enter its most protected organ.
The ASIA syndrome: basic concepts (2018) —This review paper presents the concept of the “autoimmune/inflammatory syndrome induced by adjuvants” (ASIA) and details how adjuvants (including aluminum salts) can trigger autoimmune or inflammatory responses in genetically predisposed individuals.
🔗 https://pmc.ncbi.nlm.nih.gov/articles/PMC7046028/Aluminum vaccine adjuvants: are they safe? (2011) — This review states that although aluminum adjuvants have been used for a long time, toxicological and pharmacokinetic data remain relatively limited, and aluminum adjuvants may potentially induce autoimmune diseases, long-term brain inflammation, and neurological complications.
🔗 https://pubmed.ncbi.nlm.nih.gov/21568886/Biopersistence and Brain Translocation of Aluminum Adjuvants of Vaccines (2015) — This study details the biopersistence of aluminum adjuvant particles, explaining that they may reach the brain through macrophages and thus be associated with delayed neurotoxic effects.
🔗 https://www.frontiersin.org/journals/neurology/articles/10.3389/fneur.2015.00004
3. The third technology — the new mRNA platform used during COVID — unleashes an entirely different kind of chaos. It instructs the body’s own cells to produce a foreign protein, causing the immune system to identify those cells as “infected” and destroy them. This “friendly fire” can occur anywhere in the body where the technology appears — in the heart, blood vessels, or nervous system — leading, in Weinstein’s words, to the “random, chaotic destruction of tissues.”
This technology represents perhaps the most serious mistake in modern biology: an experiment in which the body’s own cells are turned into biological weapons factories. Instead of delivering a harmless antigen, it introduces a genetic instruction that commands the cells to produce a foreign protein — the spike protein. At first glance, this solution seems elegant — using the cells’ own “laboratories” for production — but in reality, it is a form of suicidal programming that turns the organism against itself.
The built-in flaw: uncontrolled spread and a chain reaction of cell destruction
One of the most fundamental laws of our immune system states that if a cell produces a foreign protein, it is considered infected and must be destroyed. mRNA vaccines artificially trigger this mechanism — except that this time there is no external virus, only the body’s own previously healthy cells, which the vaccine has turned into “enemies.” The consequence is inevitable: friendly fire — a total immune war waged by the body against itself.
And the chaos doesn’t stop there. The lipid nanoparticles (LNPs) that deliver the mRNA do not stay at the injection site, as the official narrative once claimed. Pfizer’s and Moderna’s own preclinical biodistribution data, along with several independent animal studies, have shown that these LNPs travel through the bloodstream to every part of the body — the liver, spleen, heart, ovaries, and even the brain. Moreover, these tiny lipid spheres are inherently inflammatory and capable of crossing the blood–brain barrier, triggering immune activation within the nervous system.
The body as a battlefield: the logic of cell destruction and “friendly fire”
Wherever a cell takes up the genetic instruction from the vaccine, it begins to produce the spike protein. The immune system then naturally identifies that cell as infected and destroys it. This process can occur anywhere:
in the heart muscle (myocarditis),
in the blood vessel walls (vasculitis, endothelial damage),
in the nervous system (neuroinflammation, demyelination),
or in the reproductive organs (ovarian or testicular damage).
Several studies published in Nature Medicine and other leading journals have already confirmed that post-vaccination myocarditis is not a “rare and inexplicable side effect,” but a mechanically and immunologically plausible consequence of the technology itself. The scientific consensus now recognizes a causal relationship — not as a random accident, but as a direct outcome of how the technology works. The immune system reacts strongly to the spike protein produced by heart muscle cells and, following the logic of “friendly fire,” destroys the body’s own previously healthy cells. The term “inevitable” here does not mean that it happens to everyone, but that the risk of myocarditis is built into the design of the technology. Since the vaccine uses the body’s own cells as antigen factories, the potential for “friendly fire” in the heart and other organs is an inherent feature of the system, not an external or random error.
Publications in the Journal of Medical Virology have identified the mechanism of molecular mimicry: certain segments of the spike protein bear deceptive similarities to human proteins, potentially triggering autoimmune reactions in the brain, heart, and other critical tissues. This is a long-recognized immunological phenomenon that is now being intensively studied in relation to both COVID-19 and the vaccines. Numerous studies, using computational analysis, have identified specific amino acid sequences in the spike protein that show high similarity to key human proteins (such as those in the heart muscle, nervous system, or blood coagulation pathways). This does not mean that every autoimmune case is caused by this mechanism, but rather that science has identified a potential “weapon” — the misleading protein segments — that provide a biologically plausible explanation for the autoimmune phenomena observed after vaccination.
Pandora’s box has been opened
mRNA technology intervenes at the level of biological identity. Any cell that executes a foreign genetic code is no longer itself. When the immune system recognizes and destroys these cells, it is in fact dismantling the body’s own structure. This is why this system can be called the most destructive technology ever unleashed upon the human body.
The main flaw of live virus vaccines was genetic instability.
The flaw of inactivated virus vaccines was the uncontrolled immune panic caused by adjuvants.
But in the case of mRNA, it is the very code of life itself that becomes the weapon.
This is no longer medicine — it is self-destruction beyond the bounds of biological experimentation, creating chaos at the deepest level of the body in the name of protection.

Based on Dr. Weinstein’s reasoning, the conclusion is clear: since no medical product can ever be 100% safe — and all three vaccination technologies carry serious built-in risks — forcing them upon the entire population, especially children, cannot be justified by individual benefit. This compels the authorities to elevate their argument to a higher level: the intangible notions of the “common good” and social responsibility.
This is where the myth of herd immunity enters the picture — as the primary moral and legal shield of coercion. Now, let us dismantle that shield, layer by layer.
The false illusion of herd immunity
First layer: the theoretical collapse of herd immunity – the leaky and short-lived shield
The theory is based on the idea that a vaccinated individual represents a “dead end” for the pathogen — meaning they cannot transmit the infection. However, modern vaccinology knows very well that this is not true for most vaccines.
The biological reality: Childhood vaccines (DTaP, MMR, etc.) are administered intramuscularly. This triggers a strong systemic immune response in the bloodstream, which effectively protects against severe, complicated forms of disease. This is the strong wall of the fortress. However, most pathogens (for example, the bacterium causing whooping cough) enter the body through the nasal and throat mucosa — the gate of the fortress. Intramuscular vaccines do not create effective local mucosal immunity at this “entry point.”
The harsh consequence: Because the gate remains unguarded, the pathogen can settle and multiply on the vaccinated child’s mucous membranes. The child may not become seriously ill, but through sneezing or coughing can still transmit the pathogen to others. The vaccinated person thus becomes an asymptomatic carrier and transmitter of the virus.
With this, the very first and most crucial pillar of the herd immunity theory — the idea of a “shield” that prevents transmission — collapses immediately.
The second collapse: Time and waning immunity – the statistical sleight of hand
But the problems with the model don’t end there. Let’s assume the impossible: that vaccines provide perfect, sterilizing immunity. Even then, a second condition must be met — the vast majority of the population would have to remain continuously protected. In reality, this has never been true, not for a single moment.
The expiration date: The immunity provided by most vaccines does not last forever. Within a few years, or at most a decade, it weakens significantly. A child vaccinated at age five no longer has the level of protection required by the model by the time they are twenty-five.
The missing boosters: Only a tiny fraction of adults over 18 regularly receive booster shots for childhood diseases.
Generational differences: Today’s 40- to 50-year-old parents received only a fraction of the vaccines that appear in today’s immunization schedules.
The statistical illusion: The proudly proclaimed “95% vaccination rate” is a statistical trick. This figure applies only to the youngest age groups — preschool and early school-age children. It says nothing about the immunity of teenagers, young adults, middle-aged people, or the elderly, who together make up 80–90% of society.
Thus, the so-called shield of herd immunity is not only full of holes (since vaccinated people can still transmit disease), but it is also a small, temporary shield that covers only a narrow segment of the population and only for a short time. The justification for mandates — that a vaccinated child is part of a shield protecting the entire society — is therefore a doubly unfounded, scientifically untenable claim.
Second layer: the global experiment – the mRNA propaganda and the slap of reality
If anyone still had doubts about the above theory, the COVID-19 pandemic proved it in a real-time, global experiment. The propaganda blared from every channel: “The vaccine stops the spread. Get vaccinated to protect the community!”
The exposure of the lie: The entire world witnessed that this was simply not true. Both vaccinated and unvaccinated people became infected and spread the virus. The “shield” did not exist.
The verdict of the Cleveland Clinic study: A large-scale study involving tens of thousands of healthcare workers not only confirmed this but turned the official narrative completely upside down. The conclusion was shocking: the more mRNA shots a person had received, the higher their likelihood of getting sick. Those repeatedly vaccinated not only failed to stop transmission but, statistically, became more frequent carriers and spreaders of the virus.
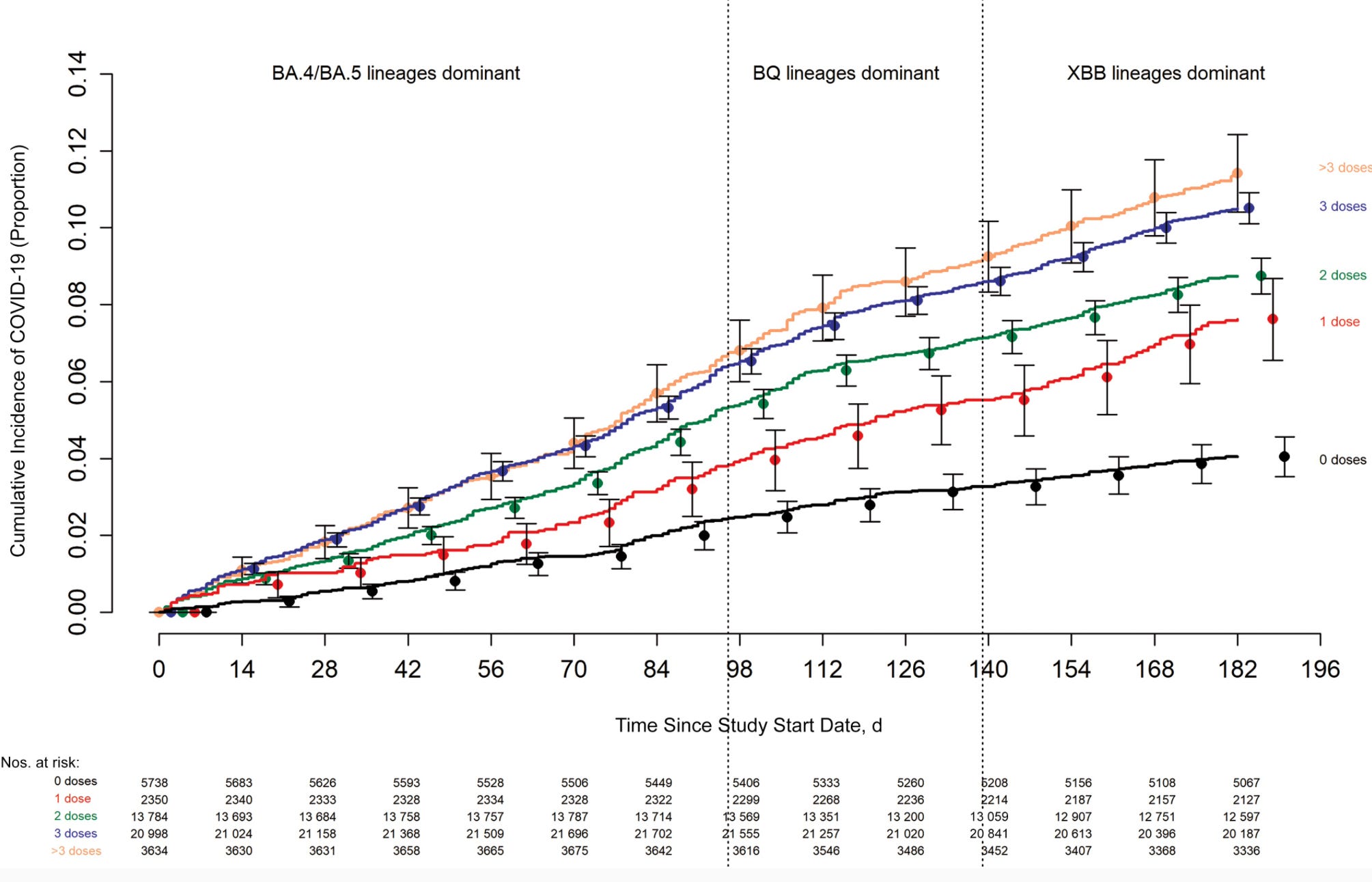
On what basis can we believe that childhood vaccines made with decades-old technology create an impenetrable communal shield, when the most modern, so-called cutting-edge vaccines not only fail to do so but, according to the evidence, may actually achieve the opposite?
Third layer: the falsification of history – the true architects of success
The other cornerstone of pro-vaccine propaganda is the oversimplified portrayal of history: “Vaccines eradicated deadly childhood diseases.” This half-truth, however, hides the real essence of what happened.
The real heroes: In the 19th and 20th centuries, mortality and morbidity rates from infectious diseases such as measles, diphtheria, and whooping cough had already declined dramatically—by more than 90%—decades before the introduction of mass vaccination programs. The true driving forces behind this success were improved hygiene, sanitation, clean drinking water, and better nutrition. Vaccines are often portrayed as the firefighter who extinguished the blaze, when in reality, the fire had already been reduced to embers—the heavy lifting had been done by public health infrastructure and rising living standards.
The control group: History itself provides the control group. Diseases for which no vaccines ever existed—such as scarlet fever or typhoid—also declined in the same period. This clearly demonstrates that improved living conditions, not a single medical intervention, were the decisive factor.
Thus, the moral argument that “you owe it to history, therefore you must vaccinate” rests on a false historical premise.
In more detail on this topic:

Fourth layer: the silenced cost – the silent epidemic of chronic disease
And here we arrive at the most uncomfortable question. While infectious diseases have declined, a new, silent epidemic has taken their place.
The parallel charts: Over the past 40–50 years, the number of mandatory childhood vaccinations has multiplied (from a few shots to several dozen injections). In parallel, the number of chronic diseases — autoimmune disorders, allergies, asthma, and neurocognitive impairments — has skyrocketed among children.
The autism tragedy: The most striking example is autism. A few decades ago, it affected one in 10,000 children; today, that ratio has changed dramatically — according to some surveys, one in every 24–30 children is diagnosed. This cannot be explained merely by “better diagnostics.” It is a real, devastating epidemic.
In Search of the Silenced Truth – The Film the Authorities Never Wanted to Be Made
MAGYAR VERZIÓ IDE KATTINTVA OLVASHATÓ!

Although the official stance claims that correlation does not imply causation, a responsible public health system would have the duty to investigate this alarming parallel — not sweep it under the rug dogmatically.
If there is a suspicion that one public health intervention (the ever-increasing number of vaccinations) may be contributing to another, perhaps even more serious public health catastrophe, then any moral justification for coercing that intervention collapses entirely.
Epilogue: coercion is the language of power, not of science
If we look honestly at the arguments, the justification for mandatory vaccination based on the so-called “greater good” collapses like a house of cards:
Herd immunity is flawed even in theory, because the vaccinated can still transmit disease.
Modern mRNA vaccines have proven their failure in practice.
The historical narrative of victory over disease is false, because the decline had already occurred almost entirely before vaccines were introduced.
The growing number of vaccines parallels a rise in chronic illnesses, raising the question of mass harm.
Thus, states are forcing parents to uphold a social contract whose every point, as we have seen, is open to question. The original, legitimate purpose of vaccination was to protect the individual against severe, complicated diseases.
But where the possible benefit belongs to the individual, the freedom to decide — based on complete and uncensored information — must also belong to the individual. Especially because the effects can last a lifetime.
Of course, it is important to understand: those who argue today in favor of maintaining mandatory vaccinations are not all acting out of bad intent. Yet it would be naive to believe that the system runs purely on good faith. At the top of the pyramid of dogma stand those who have a direct material and power interest in maintaining the status quo. They are the ones who profit from the impossibility of questioning, who actively suppress inconvenient research findings, and who use the noble idea of the “greater good” as a shield to protect profit and control.
The vast majority, meanwhile, live within this deliberately constructed informational bubble. Their actions are not driven by malice but by the absence of questioning. They have never asked themselves: do I truly know what I think I know — or do I merely believe, comfortably, what I have been told from above?
Yet now, in the age of chronic disease epidemics, it is more important than ever for anyone in a position of decision-making to take a step back from dogma and:
read,
ask questions, research,
and dare to doubt.
This debate is not about enemies — it is about courage. About the people who are brave enough to face uncomfortable truths. Because the future of our children and grandchildren now depends on how many choose thinking over blind obedience.
As I wrote at the beginning, this is not an indictment but an invitation to honest dialogue with all those who hold responsibility for our children’s health — doctors, policymakers, politicians, and journalists. This debate is not about intent. Most of those who keep the system running act according to their best convictions: they want to help, based on the information they have so far accepted as true.
The real question is whether the epidemic of chronic diseases — autoimmunity, allergies, neurological disorders — the silent tragedy of our generation, represents an even greater and more insidious threat. And whether it is we ourselves who have created a fatal connection between the two.
Of course, if we look only at the statistics, we remain blind — we fail to see the human being behind the numbers. In a statistic, a single child’s permanent health damage may be considered an acceptable “collateral loss.” But for that one child and their family, that single case is a one-hundred-percent catastrophe. Statistics show the numbers — but reality lives in our homes.
That is why this appeal is not about asking people to believe us. It is about asking them to believe in the noblest principles of their own professions:
that the doctor should heal with conscience,
the scientist should question without fear,
the decision-maker should weigh with humanity,
and the journalist should dare to speak even what is uncomfortable.
In science, there are no settled questions — only temporary theories that must be continually tested. And if the results, however uncomfortable, are supported by facts, then the previous position must be changed — that is science, not blind faith.
Dare to read the studies — even those outside the mainstream — that point to the built-in flaws of these technologies, the neurotoxicity of adjuvants, or the links between chronic inflammation and vaccination.
And dare to ask the hardest question a responsible person can ask themselves:
What if, in the name of protection, we are doing more harm than good? Asking this question does not make anyone “anti-vaccine” or “anti-science.” On the contrary — not asking it is what makes someone unscientific.
The strategy of those at the top of the pyramid is timeless: turn the people against one another. The tools and groups change—religions, ideologies, wars; today it is the vaccinated and the unvaccinated, those who support mandates or those who support free choice. The goal, however, is the same: that our energy be consumed in fighting one another. That we turn our attention to each other, not to them. For as long as we search for the enemy next door, we will never see who built the walls between us. This is the oldest formula of domination: divide and rule.
Yet all of our time here is finite. And when the final moment comes, when we look into the mirror, only one question will remain:
did we do everything we could for the future of our children and grandchildren?
It will never matter what others did for us — only what we did for others. Because in truth, we are all one — and that responsibility can never be shifted onto anyone else when we look back on our past.
